We have endeavoured to gain permission, where possible, to host these tasks and questionnaires. If you believe we are hosting something improperly, please let us know.
For similar repositories see:
I also have an example University of Surrey Information Sheet & Consent Form, please email me for me to share it with you.
And remember Gorilla has a Demos & Examples as well as Sample Tasks, Questionnaires & Experiments and great Tutorials
Gorilla Data, is downloaded as a .csv file, and requires some level of data tidying or analysis. There is a nice tutorial on data processing using R and tidyverse .
In addition, there is also this GitHub repository, which has example R scripts for data processing
Questionnaires
Tasks
Example Experiments
General & Head-Injury Related
Built with Questionnaire Builder 1
A questionnaire measure of self-reported failures in perception, memory, and motor function. For more details, see reference
CFQ Score is just summed up:
For more information on scoring see here
There is an example R Analysis script in this GitHub repository, which (amongst other questionnaires/tasks) codes for the analysis of this task. Look for the CFQ section (should be clearly marked)
Creative Commons Attribution-NonCommercial (CC BY-NC)
Broadbent, D.E., Cooper, P.F., FitzGerald, P., & Parkes, K.R. (1982). The Cognitive Failures Questionnaire (CFQ) and its correlates. British Journal of Clinical Psychology, 21, 1-16.
https://www.ncbi.nlm.nih.gov/pubmed/7126941/
Built with Questionnaire Builder 1
A simply applied quantitative assessment of handedness. For more details, see reference.
To score:
Creative Commons Attribution-NonCommercial (CC BY-NC)
R. C. Oldfield, “The assessment and analysis of handedness: the Edinburgh inventory,” Neuropsychologia, 1971, Vol. 9, No. 1, pp. 97-113.
https://www.sciencedirect.com/science/article/abs/pii/0028393271900674
Built with Questionnaire Builder 1
A simple, self-administered questionnaire which is shown to provide a measurement of the subject's general level of daytime sleepiness. For more details, see references.
And initial paper can be found here.
Creative Commons Attribution (CC BY)
Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep, 1991; 14: 50-55.
https://www.ncbi.nlm.nih.gov/pubmed/1798888
Epworth Sleepiness Scale
http://epworthsleepinessscale.com/about-the-ess/
Built with Questionnaire Builder 1
A self-assessment scale developed for detecting states of depression and anxiety in the setting of an hospital medical outpatient clinic. For more details, see reference.
To score:
Scored 3 - 2 - 1 - 0:
Scored 0 - 1 - 2 - 3:
Creative Commons Attribution-NonCommercial (CC BY-NC)
Zigmond & Snaith (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica. 67 (6): 361-370
https://www.ncbi.nlm.nih.gov/pubmed/6880820
Built with Questionnaire Builder 1
A 22-item self-report measure that assesses subjective distress caused by traumatic events. For more details, see reference.
To Score:
Creative Commons Attribution-NonCommercial (CC BY-NC)
Weiss, D. S., & Marmar, C. R. (1996). The Impact of Event Scale - Revised. In J. Wilson & T. M. Keane (Eds.), Assessing psychological trauma and PTSD (pp. 399-411). New York: Guilford. (NOTE: Includes measure in its entirety.)
https://www.ptsd.va.gov/professional/assessment/adult-sr/ies-r.asp
Built with Questionnaire Builder 1
To momentarily assess a respondent's propensity to fall asleep. For more details, see reference.
This one has 10 steps and more labels, like in Baulk et al 2001 "Driver Sleepiness—Evaluation of Reaction Time Measurement as a Secondary Task"
Creative Commons Attribution-NonCommercial (CC BY-NC)
Akerstedt T, Gillberg M. Subjective and objective sleepiness in the active individual. Int J Neurosci. 1990 May;52(1-2):29-37
https://www.ncbi.nlm.nih.gov/pubmed/2265922
Built with Questionnaire Builder 1
To momentarily assess a respondent's propensity to fall asleep. For more details, see reference.
This is the original one that has 9 steps labeled only on odd numbers.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Akerstedt T, Gillberg M. Subjective and objective sleepiness in the active individual. Int J Neurosci. 1990 May;52(1-2):29-37
https://www.ncbi.nlm.nih.gov/pubmed/2265922
Built with Questionnaire Builder 1
An English language self-assessment Morningness-Eveningness questionnaire which categorises people into Morning, Evening and Intermediate type. For more details, see reference.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Horne, JA, Östberg O (1976). "A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms". International Journal of Chronobiology. 4 (2): 97–110.
https://www.ncbi.nlm.nih.gov/pubmed/1027738
Built with Questionnaire Builder 1
A self-rated questionnaire which assesses sleep quality and disturbances over a 1-month time interval. Nineteen individual items generate seven "component" scores: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. The sum of scores for these seven components yields one global score. For more details, see reference.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Research. 1989;28:193–213.
https://www.ncbi.nlm.nih.gov/pubmed/2748771
Built with Questionnaire Builder 1
A questionnaire to measure the post-concussion symptoms (PCS) often reported by patients after mild traumatic brain injury (mTBI). For more details, see references.
To score, just add up values of each item on 0 - 1 - 2 - 3 - 4 scale:
Some studies also look at the answers split into RPQ-3 and RPQ-13. See Eyres et al (2005) Clin Rehab 19(8):878-87.
There is an example R Analysis script in this GitHub repository, which (amongst other questionnaires/tasks) codes for the analysis of this task. Look for the RPQ section (should be clearly marked)
Creative Commons Attribution-NonCommercial (CC BY-NC)
King NS, Crawford S, Wenden FJ, Moss NE, Wade DT. The rivermead post concussion symptoms questionnaire: a measure of symptoms commonly experienced after head injury and its reliability. J Neurol. (1995) 242:587–92.
https://link.springer.com/article/10.1007%2FBF00868811
Built with Questionnaire Builder 1
A questionnaire to measure the post-concussion symptoms (PCS) on control populations without head injury for general population-level symptom report. For more details, see references.
Based on the RPQ (King et al (1995), see references) and used in Sterr et al (2006); Dean et al (2012) (see references)
To score, just add up values of each item on 0 - 1 - 2 - 3 - 4 scale:
There is an example R Analysis script in this GitHub repository, which (amongst other questionnaires/tasks) codes for the analysis of this task. Look for the RPQ section (should be clearly marked)
Creative Commons Attribution-NonCommercial (CC BY-NC)
Sterr, A., Herron, K. A., Hayward, C., & Montaldi, D. (2006). Are mild head injuries as mild as we think? Neurobehavioral concomitants of chronic post-concussion syndrome. BMC Neurology, 6, [7].
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1382265/
Dean PJ, O'Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26(1):14–26
https://pubmed.ncbi.nlm.nih.gov/22107176/
King NS, Crawford S, Wenden FJ, Moss NE, Wade DT. The rivermead post concussion symptoms questionnaire: a measure of symptoms commonly experienced after head injury and its reliability. J Neurol. (1995) 242:587–92.
https://link.springer.com/article/10.1007%2FBF00868811
Built with Task Builder 1
2 Blocks of 12 practise trials, one without cueing, one with cueing (making the 24 trial full feedback practise block of Fan et al).
4 Blocks of 48 task trials (12 without cueing, 12 with dual asterisk cue [alerting], 12 with central asterisk [alerting] cue, 12 with one asterisk [orienting]) NB: Fan et al had 3 blocks of 96 trials. We split this to smaller blocks to aid in online delivery/focus
Done within the script tab:
Not yet fully operationalised:
There is an example R Analysis script in this GitHub repository, which (amongst other questionnaires/tasks) codes for the analysis of this task. Look for the ANT section (should be clearly marked)



Creative Commons Attribution-NonCommercial (CC BY-NC)
Fan et al (2002), Testing the Efficiency and Independence of Attentional Networks, Journal of Cognitive Neuroscience, 14:3, pp340-347
https://www.ncbi.nlm.nih.gov/pubmed/11970796
ANT Task Download
https://www.sacklerinstitute.org/cornell/assays_and_tools/ant/jin.fan/
Built with Task Builder 1
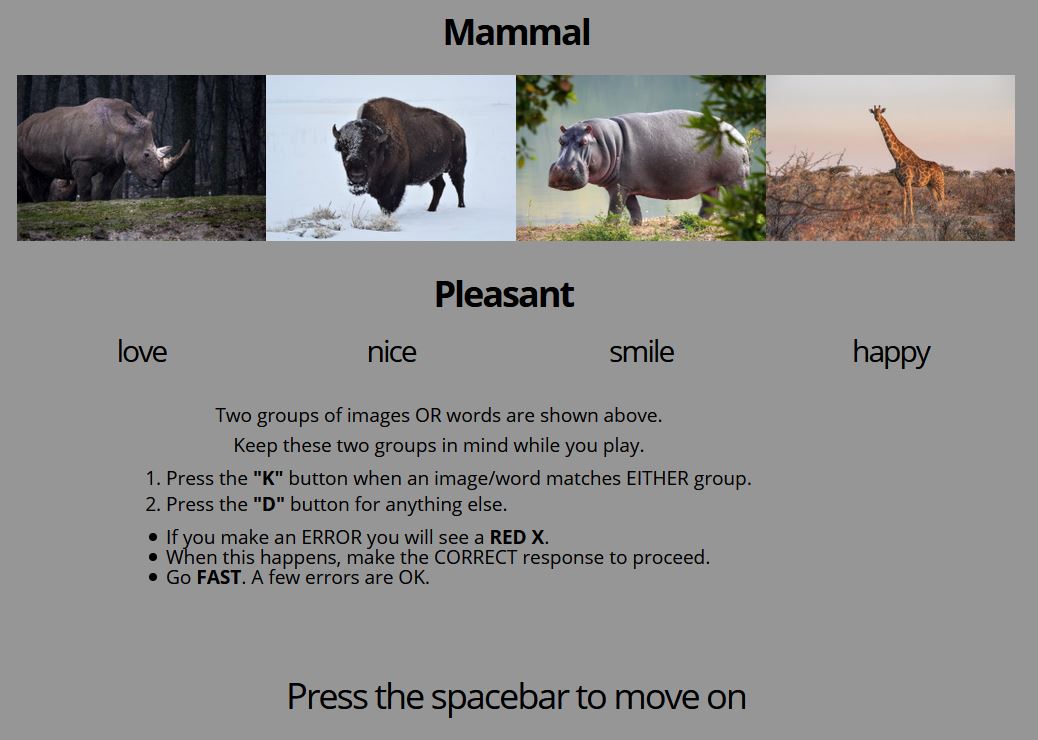
Brief Implicit Association Test (B-IAT) as conceived by Sriram & Greenwald (2009), with class-based stimuli adaptation by Adam McNamara.
NB: This task is only to be used as an example structure/setup for an B-IAT task, and should not be run as an experiment in its current form. The original image stimuli for this task have been removed to prevent over-use of stimuli. They have been replaced with free-to-use images from Pixabay (https://pixabay.com/), and the images used have not been determined to be representative of the categories nor scientifically matched/determined.
Adapted for children to 4 blocks of 20 stimuli (12 Images, 8 words [with sound]).
There is a practise block of 16 stimuli. This consists of 2 * 8 stimuli presentations, where the stimuli are randomly picked (without replacement) from the 16 possible stimuli (8 images, 8 words).
There is an example R Analysis script in this GitHub repository, which analyses the data according to Nosek et al 2014.

Creative Commons Attribution-NonCommercial (CC BY-NC)
Sriram & Greenwald (2009). The Brief Implicit Association Test. Experimental Psychology, Vol. 56(4):283–294. DOI: 10.1027/1618-3169.56.4.283
https://faculty.washington.edu/agg/pdf/Sriram&Greenwald.BIAT.2009.pdf
Nosek BA et al. (2014) Understanding and Using the Brief Implicit Association Test: Recommended Scoring Procedures. PLoS ONE 9(12): e110938. https://doi.org/10.1371/journal.pone.0110938
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0110938
Nosek, B. A., Greenwald, A. G., & Banaji, M. R. (2007). The Implicit Association Test at age 7: A methodological and conceptual review (Pp. 265–292). In J. A. Bargh (Ed.), Automatic processes in social thinking and behavior. Psychology Press.
https://faculty.washington.edu/agg/pdf/Nosek%20&%20al.IATatage7.2007.pdf
Greenwald et al. (1998). Measuring Individual Differences in Implicit Cognition: The Implicit Association Test. Journal of Personality and Soclal Psychology 1998, Vol. 74, No. 6, 1464-1480
https://faculty.washington.edu/agg/pdf/Gwald_McGh_Schw_JPSP_1998.OCR.pdf
Built with Task Builder 1
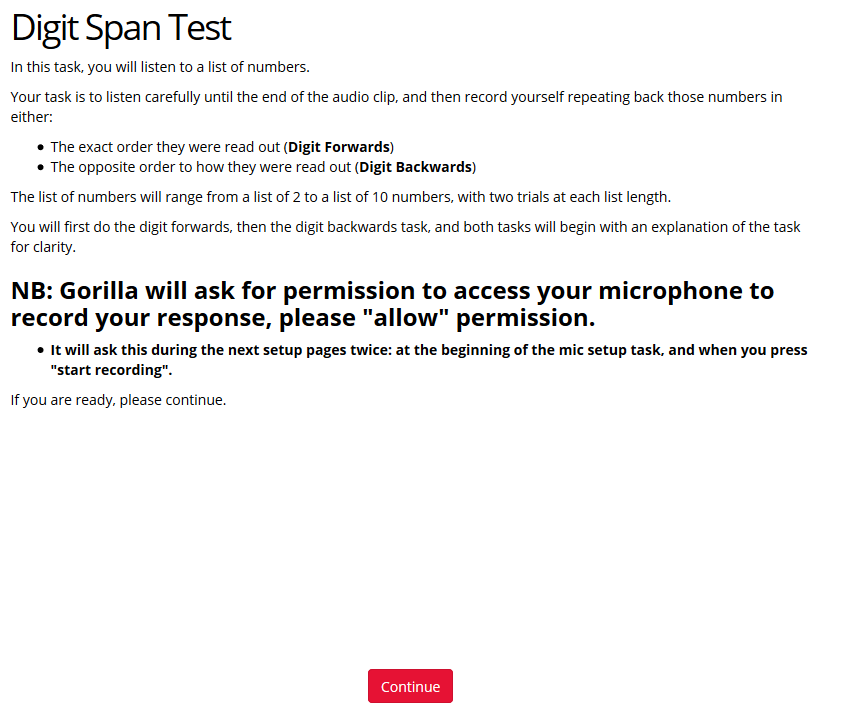
This test is adapted from Mark Turner & Jacky Ridsdale 2001's assessment procedure for specialist teachers to investigate verbal memory difficulties in children’s learning.
There are two different versions of the spreadsheet/digit lists (List A & List B), so a pre-post intervention task can be run and counterbalanced, without any learning effects.
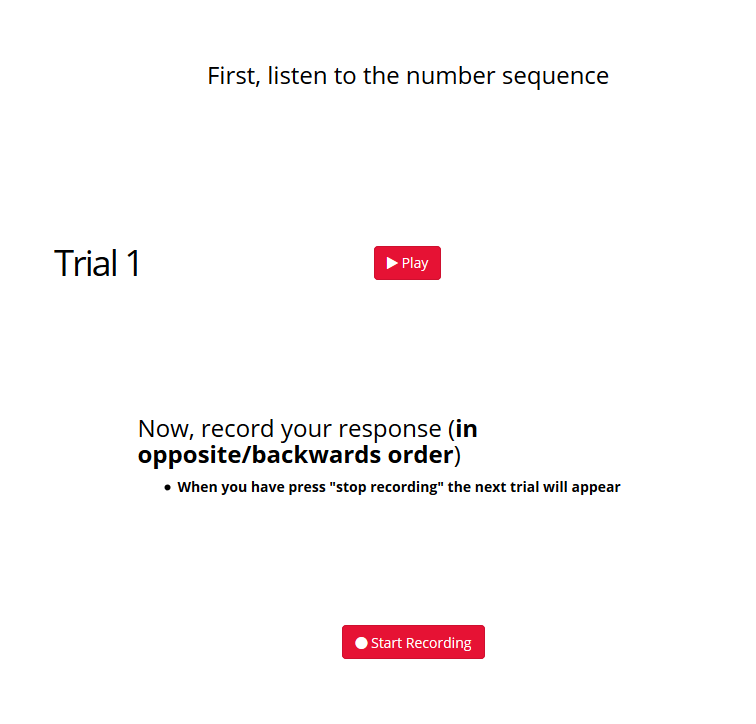
This task requires the use of Audio (to play the lists) and a microphone (to record your response), and has audio and microphone test screens to ensure participants are aware of this, and have the correct levels to do the task. It also allows participants the ability to "allow" Gorilla permission to use the microphone during the test, so this does not impact recording of the task.
You would ordinarily administer this until a participant fails on both trials at a particular digit span. This online test will collect all digit spans as it records the audio from the participant, and online analysis of whether this is correct or not is not possible. Therefore, *when scoring you need to only count up to the trial where a participant failed both trials, and discount any further trials.
Scoring:
Standard scores & percential equivalents are available from Mark Turner & Jacky Ridsdale 2001

Creative Commons Attribution-NonCommercial (CC BY-NC)
Turner, M., and Ridsdale, J. (2004). The Digit Memory Test. Available online at: https://www.dyslexia-international.org/content/Informal%20tests/Digitspan.pdf (accessed June 25, 2016).
https://www.dyslexia-international.org/content/Informal%20tests/Digitspan.pdf
Turner, M., and Ridsdale, J. (2004). The Digit Memory Test. Available online at: http://www.eleanorhick.co.uk/images/MorningTraining/AMSpring2018/Digitspan.pdf(accessed March 24, 2020).
http://www.eleanorhick.co.uk/images/MorningTraining/AMSpring2018/Digitspan.pdf
Built with Task Builder 1
This test is adapted from Mark Turner & Jacky Ridsdale 2001's assessment procedure for specialist teachers to investigate verbal memory difficulties in children’s learning.
There are two different versions of the spreadsheet/digit lists (List A & List B), so a pre-post intervention task can be run and counterbalanced, without any learning effects. NB: Digit Forwards is always presented before Digit Backwards in both these lists.
This is a visual & text entry version of the audio one above. Text is on-screen for 500ms, with 500ms "gap" between numbers, meaning numbers presented every 1s as per "bedside" clinical test.
This task goes to the end of the condition (Digit Forwards or Digit Backwards) if a participant fails on both trials at a particular digit span. (Thanks to Dan Brady, University of Reading for starting coding this exit condition)
Scoring:
Standard scores & percential equivalents are available from Mark Turner & Jacky Ridsdale 2001
NB: it is possible to "cheat" on this task (and the audio one above). It has been brought to my attention by another researcher that their participants were writing down the numbers on paper as they came up, to enter in later. Although difficult, this is possible if people are quick at writing whilst looking at the screen. Alternatively, people can type out the numbers for the digit backwards into the text entry box, and then reverse them, deleting the initial part and getting the answer correct as if it was a digit forwards task. Both of these strategies (and likely more) can result in high, if not 100%, performance rates. I can think of no completely satisfactory way of preventing this from happening in such an online task, but it could be screened after collection: please see Jenni Rodd's great talk on data quality online. There might be longer reaction times if people are doing these tactics, but i don't think to the extent where they wouldn't overlap with others who just take a long time to answer correctly. High performance may be an indicator, and you could add longer lists. A "catch" trial/condition where it would be impossible without doing one of these tactics (e.g. a long number to remember at beginning of experiment, and only put in at end), but this might also impact the main experiment. Observing participants when doing this may be an option, but then it might be easier just to do the simple original audio "bedside" clinical version of the task where such cheating is not possible.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Turner, M., and Ridsdale, J. (2004). The Digit Memory Test. Available online at: https://www.dyslexia-international.org/content/Informal%20tests/Digitspan.pdf (accessed June 25, 2016).
https://www.dyslexia-international.org/content/Informal%20tests/Digitspan.pdf
Turner, M., and Ridsdale, J. (2004). The Digit Memory Test. Available online at: http://www.eleanorhick.co.uk/images/MorningTraining/AMSpring2018/Digitspan.pdf(accessed March 24, 2020).
http://www.eleanorhick.co.uk/images/MorningTraining/AMSpring2018/Digitspan.pdf
Built with Task Builder 1
Based on Kahan & Hely (2008).
This allocates colour to the word on a trial by trial basis (i.e. the colour is not strictly counterbalanced across conditions, and number of trials with each colour is not strictly counterbalanced).
Original paper was voice response. This uses keys R, G, B, Y (for Red, Green, Blue, Yellow).
NB: this has not been run on any experiment, and is to be used a first draft version/example to be checked/adapted only.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Kahan, T.A., Hely, C.D. The role of valence and frequency in the emotional Stroop task. Psychonomic Bulletin & Review 15, 956–960 (2008). https://doi.org/10.3758/PBR.15.5.956
https://link.springer.com/article/10.3758/PBR.15.5.956
Built with Task Builder 1
Based on versions of the n-Back task made for Dean & Sterr (2013) & Dean at al (2015) [see references], adapting to do just 2-Back and 4-Back.
2 Blocks of 8 practise trials, one for 2-Back (always first), one for 4-Back (always second).
10 Blocks of 30 task trials (10 Target, 20 non-Target), 5 each of 2-Back and 4-Back.
Block order randomised, however, Order/stimuli within each block is hard coded in spreadsheet (see below)
Participants must press for** both** target and non-target.
Done within the script tab:
There is an example R Analysis script in this GitHub repository, which (amongst other questionnaires/tasks) codes for the analysis of this task. Look for the n-Back section (should be clearly marked)

Creative Commons Attribution-NonCommercial (CC BY-NC)
Dean & Sterr (2013), Long-term effects of mild traumatic brain injury on cognitive performance, Frontiers in Human Neuroscience, 7:30
https://www.frontiersin.org/articles/10.3389/fnhum.2013.00030/full
Dean at al (2015), Multimodal imaging of mild traumatic brain injury and persistent postconcussion syndrome. Brain and Behaviour, 5(1): 45-61
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4321394/
Built with Experiment
Example experiment containing:
With an example of branching dependent on previous result.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Consent to contact for taking part in further studies after initial screening
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Example debrief, after screening, and before main task.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Demographics for concussion/mild traumatic brain injury (mTBI) study with:
NB some of these options are "Personal Data" for GDPR purposes and some are "special category personal data", and you need to have a data management plan for these, and have mentioned them in the information sheet to make sure your participant is aware what you are taking, why, for how long, how you will handle it, whether and how they can remove their data, and who is responsible for the data. See University of Surrey Ethics for more details.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Head Injury Specific data for concussion/mild traumatic brain injury (mTBI) study with:
NB these options are "special category personal data" for GDPR purposes, and you need to have a data management plan for these, and have mentioned them in the information sheet to make sure your participant is aware what you are taking, why, for how long, how you will handle it, whether and how they can remove their data, and who is responsible for the data. See University of Surrey Ethics for more details.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Sports-related information for concussion/mild traumatic brain injury (mTBI) study with:
NB some of these options are "special category personal data" for GDPR purposes, and you need to have a data management plan for these, and have mentioned them in the information sheet to make sure your participant is aware what you are taking, why, for how long, how you will handle it, whether and how they can remove their data, and who is responsible for the data. See University of Surrey Ethics for more details.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Supplement & Diet-related information for concussion/mild traumatic brain injury (mTBI) study with:
NB some of these options are "special category personal data" for GDPR purposes, and you need to have a data management plan for these, and have mentioned them in the information sheet to make sure your participant is aware what you are taking, why, for how long, how you will handle it, whether and how they can remove their data, and who is responsible for the data. See University of Surrey Ethics for more details.
Creative Commons Attribution-NonCommercial (CC BY-NC)
Built with Questionnaire Builder 1
Post-Season head injury screening for concussion/mild traumatic brain injury (mTBI) study with:
NB these options are "special category personal data" for GDPR purposes, and you need to have a data management plan for these, and have mentioned them in the information sheet to make sure your participant is aware what you are taking, why, for how long, how you will handle it, whether and how they can remove their data, and who is responsible for the data. See University of Surrey Ethics for more details.
Fully open! Access by URL and searchable from the Open Materials search page